Precision Experience: What it is and Why it Matters to Healthcare Now?
Precision Experience: What it is and Why it Matters to Healthcare Now?
By: ProCARE Portal
|
August 31, 2022

By Dr. Hamlet Benyamin
The world is on the other side of the COVID19 pandemic. Healthcare systems have been challenged, and people have died during this crisis. The time for change is now. Leaders, payors, governments, patients, and the workforce agree that if the healthcare system is to survive, it must continue to change for the better. Healthcare is dealing with provider burnout, workforce shortage, and the requisite for value in healthcare delivery. We will discuss why leaders need to shape the healthcare environment precisely and how that affects the main drivers of healthcare value and purpose. The Precision Experience of patients and the healthcare workforce are critical to improving healthcare.
Crisis accelerating the evolution of healthcare is hardly a contemporary phenomenon. The Civil War ushered in a wave of progress, including care facilities, research, and new clinical technique. The War Risk Insurance Act that provides coverage for service members in the event of death or injury emerged in World War I. The Great Depression saw Henry Kaiser create a pre-paid healthcare program for workers and their families. In the 1970s, 80s, and 90s, healthcare saw the Health Maintenance Organization act of 1973, the Consolidated Omnibus Budget Reconciliation Act of 1986, and the Health Insurance Portability and Accountability Act of 1996. A crisis should not be feared but seen as an opportunity to learn and improve.
The COVID19 pandemic has joined the list of crises that have accelerated the evolution of healthcare. The polarization of the vaccine rollout, the preponderance of misinformation, the dangers to the healthcare workforce, and the desire for members of the community to be heard will be long-lasting lessons from the pandemic. In a speech to address educational disparities in 1959, Senator John F. Kennedy remarked, “When written in Chinese, the word “crisis” is composed of two characters – one represents danger, and one represents opportunity.” We are at a change point defined by the need to advance personalized care. Personalized care is the sincere attentiveness and purposeful delivery of care to patients. Quality care through evidence-based medicine and its core values of best research evidence, clinical expertise, and patient valueshas dominated medical care for the last 20 years.1 However, Precision Health and its promise to our unique patients is the future of healthcare.
Individualized healthcare is an acknowledgment that a one-shoe-fits-all approach to healthcare is deficient. Socioeconomic disparities, exposomics, and uniquely individual behaviors are guiding principles to providing personalized healthcare. Providers recognize that the care patients need and desire is unique to those patients. A discussion with family regarding end-of-life decisions and personal values contrasts with supporting decisions regarding elective surgeries that promise to improve quality of life. Similarly, populations with difficulty gaining access to healthcare need flexible and mobile care. Healthcare is reaching them rather than waiting for the converse. Frictionless vs. memorable experiences are not mutually exclusive for growth, as suggested by some research.2 A spouse who needs blood drawn for routine pre-operative testing may expect a rapid and convenient experience. However, a family discussing care plans for their loved one in the hospital may want a memorable experience defined by clarity, empathy, and shared decision-making. Patient-centered care is the recognition of the importance of patient values. Patient experience is the necessary complement to individualized medical care.

Precision health and precision medicine are mistakenly often used interchangeably. Precision medicine is “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person.”3 Precision experience is the environment that leaders shape and influence based on the patient and workforce population’s needs, values, and success. Therefore Precision Health = Precision Experience (patient and workforce) + Precision Medicine. It is worth noting that some would support precision public health as a component of precision health; however, I leave this principle to public health experts and future discussions. The patient experience is integral to the patient’s care and unique needs. This note discusses how the workforce experience also needs precision design and its direct effect on the value and purpose of healthcare.
There is abundant literature on the performance of professionals and their influence on customer satisfaction and value. Heskett’s discussion on Service-Profit Chain highlights the consumer value-satisfaction-loyalty tree gained through the internal employee experience-quality-satisfaction sequence.4 An employee whose environment promotes satisfaction and loyalty impacts the customers it serves positively. Heather Laschinger identified nursing work environments and their direct outcome on patient safety.5 Physician wellness, a reflection of the work environment, impacts the performance of a healthcare system.6 Acknowledging dynamic and variable environments is essential to address the climate of the healthcare workforce.
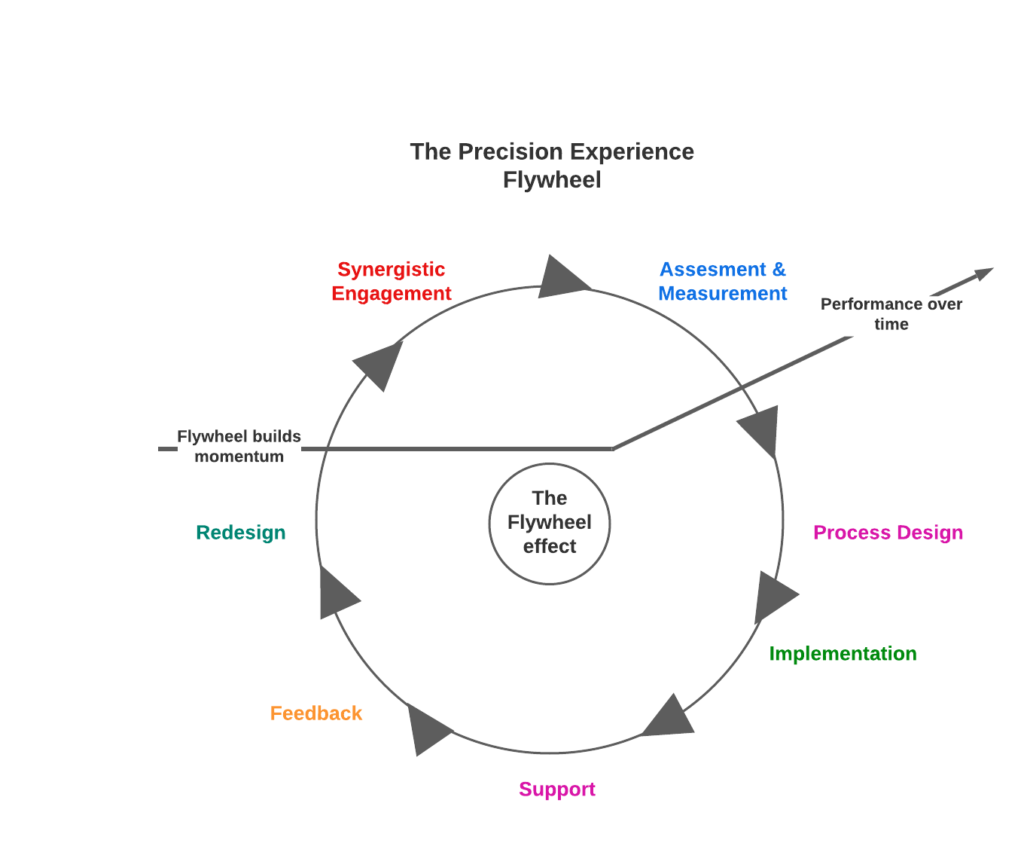
The healthcare work environment is not uniform across the country. The environment is a continuum that changes in form and expectation. Preventative care, acute care, elective care, and public health initiatives provide unique and dynamic environments. The Precision Experience for the workforce is defined by examining multiple dimensions in a loop process, including; assessment and measurement, process design, implementation, support, feedback, redesign, and synergistic engagement. The most challenging of these steps is process design. Leadership can design a series of actions to promote an overall goal; however, the method often does not promote the optimal environment. An endpoint to a failed environment is provider burnout and workforce shortage.
Provider burnout is well recognized as a syndrome driven by the failure of the work environment. A blindness to the work environment sabotages the overall goal of delivering high-value care to patients. Christina Maslach has pioneered research in the predictors and measurement of workplace burnout. The Maslach Burnout Inventory (MBI) has become the definitive measure of workplace burnout. The MBI dimensions of emotional exhaustion, depersonalization, personal accomplishment, cynicism, and professional efficacyparallel Dan Pink’s intrinsic motivation framework, including mastery of skills, autonomy as a self-directed choice, and a purpose for one’s work.7,8 Our endeavor as leaders should be a process that nurtures motivation and mitigates burnout. The National Academy of Medicine discussion paper offers a concise discussion of the domains and practices to promote well-being. These domains are defined as; “(1) organizational commitment, (2) workforce assessment, (3) leadership (including shared accountability, distributed leadership, and the emerging role of a chief wellness officer [CWO]), (4) policy, (5) efficiency of the work environment, and (6) support.”9 Burnout is a national problem that some studies suggest that 50% of providers suffer from.10 In addition, a recent MIT Sloan research article described the effects of culture and environment on the Great Resignation.11 The importance of addressing the environment prevents a domino effect characterized by Broken Window Theory, popularized by social scientists James Wilson and George Kelling12. As problems go unattended in an environment, people’s attitudes toward the environment deteriorate and lead to more problems. To solve this, we must ask what an optimal work environment is. What processes promote wellness and coherence with performance? What framework encompasses self-satisfaction and performance?
Precision experience for the healthcare workforce should aim to achieve a state where people feel their best and perform their best. The seminal work of Mihaly Csikszentmihalyi has studied the state of FLOW. As we examine the characteristics of FLOW, we see why processes grounded in those principles are best suited to provide an experience valuable in healthcare. Paul Bataldon’s quote, “Every system is perfectly designed to get the results it gets,” is a critical reflection.13 A precise, purposeful design gets the best performance and sense of self-satisfaction. FLOW has been studied in athletes, artists, chess grandmasters, and physicians. Csikszentmihalyi repeatedly references the state that a surgeon feels where the process of operating and being part of a successful team brings self-satisfaction. The state becomes compelling enough to perform the process for the sake of the process itself as much as performing for the directed goal. Csikszentmihalyi discusses that the goals drive the process; however, in FLOW, the process begins to drive the goal. Suppose healthcare can shift to meeting the expectations of our patients and goals of high value, safe, personalized care. Why not provide that experience through a process that promises self-satisfaction and a self-fulfilling prophecy?
Key performance indicators are rampant, yet key FLOW metrics are absent. There are six Csikszentmihalyi FLOW dimensions that leaders can create, leading to fulfilling goals for the patient and the workforce. These characteristics are, confronting tasks that people can complete, concentrating on the task at hand, clear goals with challenges matched to skills, immediate feedback, deep involvement with personal motivators, and a sense of control over the action14.
The first principle is creating a task that we have a chance to be completed. A process that begins with self-defeat is destined to be doomed. For example, a provider that provides care for surgical patients in an operating room that cannot provide urgent or semi-emergent care due to room availability compromises surgical calls and timely care for the patient. Similarly, a nurse whose ratio of patient to staff exceeds what is felt safe creates a sense of inability to perform expected care. FLOW metrics can be surveyed before outcomes of burnout, anxiety, and loss of self-satisfaction with work.
The next metric cites that the provider must be able to focus and concentrate on the task at hand. Providers want to care for patients, and technology is an adjunct to the skills and motivators for patient care. However, distractors are in excess in healthcare. These distractors are labeled as “hassle factors” or “pebbles in my shoe.” Providers required to complete pre-authorizations, insurance medical director calls, and EMR entry with frequent hard stops are encountering distractors. Daniel Goleman would remind us of the difficulty of avoiding the dilemma when sensory distractors become potent emotional distractors15. Removing sensory distractors before they become emotional distractors is vital in promoting a focused environment.
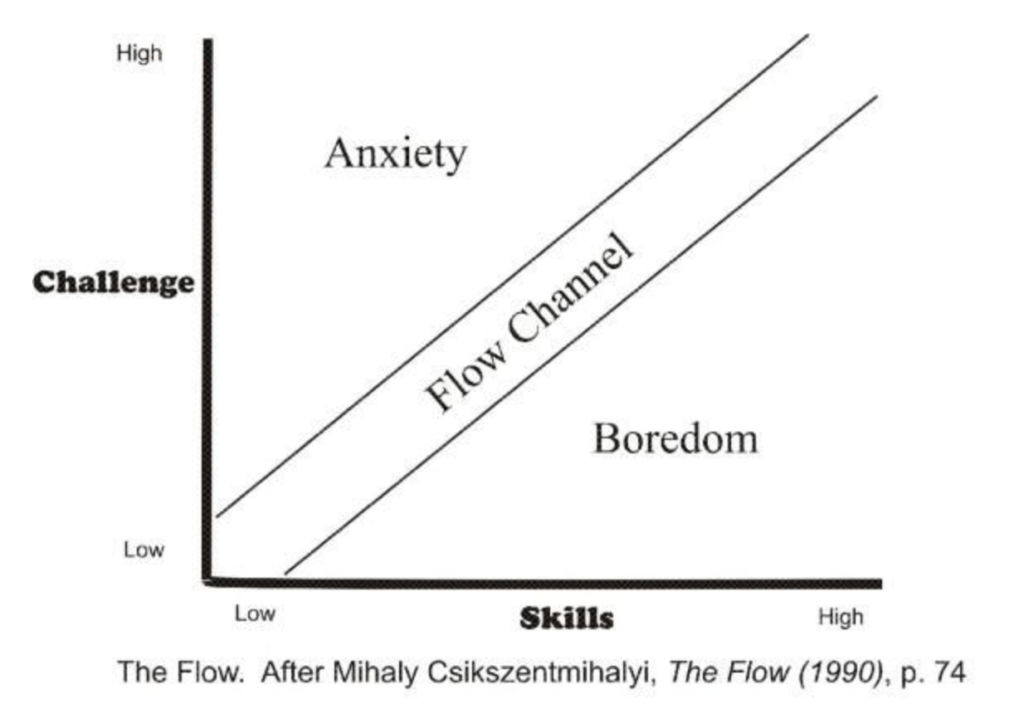
The third metric is that the task undertaken has clear goals. For example, an emergency department with increased patients leaving without treatment (LWOT) needs specific goals to target and improve. Optimizing care and reducing LWOTs is more than seeing more patients. Critical measures of time from check-in to ED room, time from room to seeing a physician, time from seeing a physician to labs, and many more goals describe improving the process. Related to this is the notion of anxiety vs. boredom in goals. Csikszentmihalyi describes the optimized state between challenge and skill to achieve an optimized state. A mismatch between the two can lead to anxiety if the challenge exceeds skill and can also lead to boredom if the skill exceeds the challenge. Both states would be a failure to optimize the environment to the abilities of the workforce.
The fourth metric involves immediate feedback. Processes that fail to provide feedback to employees risk a disconnect between action and reaction. Providers should know when their actions are on track with goals and when they are not. In an outpatient clinic, discussing the goals of the visit while utilizing a prepopulated “goals of visit” form reinforces that the needs of the patient and the visit are fulfilled. In addition, a trauma surgeon who can see the team working in concert retrieving blood draws upon patient arrival, addressing imaging being ordered, and providing updated patient vitals relative to action are engaged in a feedback loop of action and reaction. Immediate feedback of action allows a course correction to maintain the pursuit of goals.
The fifth metric defines the process as linked to a deep-seated effort with a strong motivator. A requisite in healthcare is to have an altruistic need to help others. Identifying the personal motivator and creating a task that is congruent with this is essential. For example, the hospitalist may enjoy providing care in the acute setting but particularly enjoys preparing patients’ expectations regarding their hospital stay upon admission. That hospitalist enjoys admitting patients to the hospital as patients embark on their care journey. Conversely, the provider may enjoy discussing with family social issues that prevent access to care to prevent future hospitalizations. This hospitalist would be better served guiding patients through their care as preparations are made to transition to the next level of care for the patient. In addition, surgeons who enjoy emergent surgeries in the hospital and have embraced acute hospital care may choose to be surgicalists rather than outpatient specialists. The environment created should strengthen the sense of self and reinforce intrinsically rewarding values.
The sixth metric is having a sense of control. To be more specific, the ability to exercise control empowers people. Providing care in healthcare can be stressful, time-consuming, and at times dangerous, but minimizing those aspects gives a sense of control. Avoiding a disconnect between demands and resources is similar. A typical example is a new initiative instituted by a system without the provider’s or workforce input. This disconnect can create a sense of “learned helplessness” that defines a state where people feel helpless to affect a stimulus. The initiative may have value or be well intended; however, without provider involvement in design and inception, a sense of inability to have a meaningful effect may overwhelm the circumstance. The ability to impact the design of a process will reinforce a sense of control over the task. If the task lacks control over inception and operation then the workforce is not empowered. Precision experience for the healthcare workforce is an opportunity to provide an environment that is both a state where people feel their best and are performing their best. Healthcare shortages and burnout reflect a deficient work environment.
Healthcare shortages and provider burnout result from the same decay in the work environment. While some legislation has been created at the state level to reward graduate programs that increase their pipelines for new local graduates, shortages continue to exist. Some healthcare systems have been motivated to create their own nursing and provider programs to help mitigate shortages, but this has been an incomplete solution. The cost of physician recruitment and start-up has ranged from $268,000-$957,000 per physician based on specialty, experience, and expertise16. The most cost-efficient method to improve shortages is to promote an environment that reduces workforce migration. A workforce that is retained will minimize shortages but also promote stability in the culture and processes that have been nurtured.
Precision experience is also essential in the continued aspiration to minimize the fee-for-service model that rewards providers for volume care instead of value. As integrated delivery networks and accountable care organizations adapt to an increased risk model, the provider and administrator population needs a positive cultural change. For example, the “payvider” is a value-based partnership between payers and providers with more control over risk management to gain a competitive advantage. The three categories of the payvider include healthcare systems creating their insurance plans, payors and providers creating a unified partnership, and insurance providers pivoting to a healthcare provider with insurance benefits.17 This transition is a good sign that systems are acknowledging the importance of creating value to reduce costs in healthcare and their willingness to take action. However, how does this change the provider experience? An experience that precisely describes the performance metrics, reimbursement models, and incentivized goals is vital to provider and organizational alignment. The culture of trust and transparency cannot be overlooked as a critical element affecting provider behavior and motivation. Technologies that provide an enterprise solution for large-scale support and adaptability to provider and healthcare system needs are emerging.
Healthcare is emerging and re-engaging after dealing with a pandemic that has strained resources and claimed precious lives. It is vital to accelerate the evolution of healthcare that delivers on its promise to patients and its workforce. A de facto healthcare experience is deficient and must be exchanged for an experience with purpose and success in mind for the patient and its supporting workforce. An engaged, motivated, supported workforce will positively affect the personal and mental well-being of the patients it aims to serve. A Precision Health paradigm will be successful when technologies of Precision Medicine are joined with the steadfast design of Precision Experience.
WORKS CITED
1. Sackett, DL Strauss et al. Evidence-based medicine: how to practice and teach EBM. 2nd ed. Edinburgh, Scotland: Churchill Livingston; 2000.
2. Williams, Luke et al. What’s the Right Customer Experience for Your Brand? Harvard Business Review. July 30, 2021.
3. Retrieved from https://medlineplus.gov/genetics/understanding/precisionmedicine/definition/
4. Heskett J, Jones T, et al. Putting the Service-Profit Chain to Work. Harvard Business Review. July-August 2008.
5. Laschinger H, and Michael P Leiter. The impact of nursing work environments on patient safety outcomes: the mediating role of burnout/ engagement. J Nurs Adm May 2006(5): 259-67.
6. Wallace PHD, Wallace et al. Physician wellness: a missing quality indicator. THE LANCET. November 2009, pp 1714-1721.
7. Maslach, C., Jackson, S. E., & Leiter, M. P. (1997). Maslach Burnout Inventory: Third edition. In C. P. Zalaquett & R. J. Wood (Eds.), Evaluating stress: A book of resources (pp. 191– 218). Scarecrow Education.
8. Pink, Dan. Drive: The Surprising Truth About What Motivates Us. Riverhead Books. April 5, 2011
9. Sinsky, Christine et al. Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being. National Academy of Medicine. November 2020. Retrieved https://nam.edu/organizational-evidence-based-and-promising-practices-for- improving-clinician-well-being/
10. Shanafelt TD, Boone S, Tan L, Dyrbye LN, Sotile W, Satele D, West CP, Sloan J, Oreskovich MR. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012 Oct 08;172(18):1377-85
11. Sull, Donald, et al. Toxic Culture is Driving the Great Resignation. Research using employee data reveals the top five predictors of attrition and four actions managers can take in the short term to reduce attrition. MITSloan Management Review. January 11, 2022.
12. Rick, Torben. Broken Organizational Culture. Corporate Culture. March 18, 2016. Retrieved https://www.torbenrick.eu/blog/culture/broken-organizational-culture/
13. MacDavey, Megan. System Redesign Part I: Why It Matters. April 25, 2018, Retrieved https:// thetowerfoundation.org/2018/04/26/system-redesign-part-i-why-it-matters-html/
14. Csikzentmihaly, Mihaly. Flow: The Psychology of Optimal Experience. Harper & Row. January 1, 1990.
15. Goleman, Daniel. Emotional Intelligence Why it can matter more than IQ. Bloomsbury Publishing. 1995.
16. Hamidi MS et al. Estimating institutional physician turnover attributable to self-reported burnout and associated financial burden: a case study. BMC Health Serv Res. 2018 Nov 27;18(1):851. doi: 10.1186/s12913-018-3663-z. PMID: 30477483; PMCID: PMC6258170.
17. Healthcare Team. The Payvider Trend: Why it is Surging and What It Means. Retrieved https://www.medialogic.com/blog/healthcare-marketing/the-payvider-trend-why-it-is- surging-and-what-it-means/. March 18, 2022
